A Committee of Nurses Have Been Tasked With Reviewing an Increase in Central Line Infections
Authors
- Medina, Alma MSN, RN
- Serratt, Teresa PhD, RN
- Pelter, Michele PhD, RN
- Brancamp, Tami PhD, CCC-SLP
Abstract
Central line-associated bloodstream infection (CLABSI) rates above the national average precipitated a quality improvement project aimed at reducing this trend. We implemented daily chlorhexidine bathing and used 4 strategies to promote a change in practice and civilisation in our medical/surgical units. These strategies include the following: (1) staff instruction, (2) leadership support, (3) resource availability, and (4) increased sensation and accountability. Since implementing these strategies, there has been a pregnant reduction in CLABSI rates in the medical/surgical units.
Article Content
BLOODSTREAM INFECTIONS are a major crusade of morbidity and increased mortality in wellness intendance and are also attributed to an increased length of stay and escalating costs.1,ii Central line use is a major hazard gene for bloodstream infections.1,3,4 More than 250 000 cases of hospital-caused bloodstream infections associated with central lines occur annually inside the United States, with only a reported eighty 000 cases occurring in the intensive care unit (ICU) setting lone.5 This estimate highlights the fact that most bloodstream infections (BSI) occur in patients who are in units other than ICUs.2,4,half dozen,7 An intervention that has recently garnered attention in decreasing bloodstream infections is the topical employ of the antiseptic chlorhexidine gluconate (CHG) every bit a means to decrease the bacterial load on the skin of patients with central venous catheters or key lines. Many studies take analyzed its efficacy in the intensive care population; support for its utilize in the not-ICU population is increasing.viii The purposes of this quality improvement (QI) project were to implement daily chlorhexidine bathing in all adult medical-surgical units and evaluate the effectiveness of this practice change in reducing central line-associated bloodstream infections (CLABSI).
BACKGROUND
The associated costs of CLABSI were $33 000 to $75 000 per case in adult ICUs in 2009.iv This does not include the reduction in reimbursement of approximately $26 000.4 Extensive enquiry has been conducted primarily in ICUs to place the associated causes of CLABSI. I cause is the patient's own skin flora contaminating the catheter during insertion and migrating to the catheter tip.ix,10 Colonization with multidrug resistant bacteria also increases the run a risk of infection of hospitalized patients.11 The Centers for Disease Control and Prevention (CDC), Society for Healthcare Epidemiology of America, and Infectious Disease Society of America have compiled testify-based strategies to assist providers with implementation and prioritization of CLABSI prevention efforts. Strategies such as appropriate site selection, mitt hygiene, maximum barrier precautions, insertion checklists, skin antisepsis, assessment of line necessity, staff education and grooming, and a line maintenance packet (a grouping of interventions aimed at the safe handling and maintenance of central lines) are considered the golden standard in infection control and prevention.v,12,13 High infection rates across the land, even so, demonstrate a need for a renewed focus on infection prevention.xiv The focus of CLABSI prevention has now shifted to the utilise of supplemental interventions such equally chlorhexidine bathing, antimicrobial-impregnated catheters, and chlorhexidine impregnated dressings, contained interventions that take shown promise in infection control and prevention.v,12,13
Chlorhexidine gluconate is a topical antiseptic widely used for both infection control and prevention. It is effective confronting a wide range of gram-positive and gram-negative leaner, yeast, and molds. It acts by disrupting cytoplasmic membranes and remains agile for hours after application.15 Studies have used preparations of both ii% to four% CHG and 2% CHG impregnated cloths to decrease skin flora and forestall BSIs in patients with fundamental lines in ICUs.3 Several studies have identified a reduction in CLABSI ranging from 32% to 87% with little to no adverse patient reactions.16-25 The utilise of two% CHG bathing is supported by the CDC every bit a category II recommendation, suggested for implementation and supported past clinical or epidemiological studies or a theoretical rationale.5,26 Some experts believe efforts directed at postinsertion catheter apply and care may have a greater impact outside the ICU-a setting where patients take more exposure to unjustified catheter days and less stringent maintenance of insertion-site dressing.27 As mounting evidence supports the utilize of CHG baths in patients with central venous catheters, an opportunity to further decrease BSI rates exists in the non-ICU population.2,4,vi,7
METHODS
The prevention of CLABSI became a superlative priority for our facility in early 2011. Later on identifying an increased facility infection rate above the national average, a task force was formed to develop a plan to reduce CLABSI rates.28 The task force consisted of the chief nurse officer, nursing directors, nursing unit managers, infection control nurses, and bedside nurses. The unit of measurement managers selected bedside nurses who were highly engaged in process improvement and were members of the unit or hospital-based shared governance commission or had cared for a patient who developed a BSI. The task force used the Plan, Practise, Check, Act model.29 The goal of the task force was to evaluate the facility's infection control and bloodstream infection prevention practices, compare practice to current CDC guidelines, develop changes in practice according to evidence-based practise, and codify a plan for continuous comeback. Table 1 presents the specific steps of the process.
 | Tabular array 1. Steps in Practice Improvement Procedure |
The facility has 946 licensed beds, 4 ICUs, and eight medical-surgical units. There are 1091 nurses employed in the facility. Thirty-4 nurses accept obtained diploma education, 473 acquaintance, 549 available'south, 32 master's, 2 doctorate in nursing practice, and ane doctor of philosophy degrees. In addition, 253 take specialty certification. In 2012, the eight medical-surgical units had fifteen 492 (counted as the number of patients with 1 or more than central lines) while the 4 ICUs had fifteen 042 primal line days. The number of CLABSI in the medical-surgical units during this time period was 20 (rate = 1.29), compared with xix in the ICUs (rate = i.26). National CLABSI median rates (per 1000 patients) for medical-surgical units range betwixt 0.0 and 0.3 and between 0.0 and 2.8 in ICUs.thirty
Change IN PRACTICE
Beginning steps
The task strength conducted a thorough review of the current CDC central line insertion and maintenance guidelines and compared them to facility practices.5 Several deficiencies were identified. First, the facility had implemented paper insertion checklists prior to this projection, merely the task force found the checklists were non used during emergent insertions, were incomplete, or not filed in the medical record. In addition, the current do of line maintenance bundling, a term used to describe the care provided to a cardinal line post-obit insertion, was not a part of the medical tape. Since transitioning to the electronic medical record 2 years earlier, documentation of compliance with central line site maintenance lacked consistency. The current process of using visual reminders, labeling the dressing or placing a sticker with the change date on the assistants tubing, was inconsistent, and the electronic medical record lacked triggers to remind nurses of required dressing changes or tubing changes, increasing the take a chance of infection.
Another identified result was not having a standardized central line insertion cart with all the necessary supplies. The job force learned that the medical-surgical units did not stock central line insertion supplies due to cost constraints. However, waiting for the supplies was time consuming; it delayed treatment and increased the risk of infection if clinicians did not utilize the recommended protective equipment. A primal line insertion cart would address these problems. Compliance with hand hygiene was also an ongoing business concern at the facility. Surveillance identified a compliance rate of only 68% when all units and disciplines were included. This was surprising as mitt sanitizer holders were situated in highly visible and accessible places within patient care areas, and mitt hygiene was office of the new employee orientation as well equally a component of the yearly online educational requirement of all clinical employees.
The task forcefulness's review revealed 5 concerns: (1) in that location was inconsistent employ of the central line preinsertion checklist, particularly when placement was emergent; (2) primal line bundling was not role of the electronic medical record so there were no triggers to remind nurses of upcoming required tasks; (3) central line maintenance was documented inconsistently; (4) in that location was lack of admission to a standardized central line insertion cart with all the necessary supplies; and (v) compliance with hand hygiene was an event. Through the work of the task force, both insertion checklists and line maintenance bundle triggers were added to the electronic medical record within a month, allowing the nurses to receive reminders for upcoming tasks and to assist in tracking compliance.
To address the lack of available supplies, fundamental line insertion carts were assembled and stationed in each of the 3 nursing towers inside the facility. Each cart was stocked with all the equipment needed to insert central lines according to exercise guidelines. A process was instituted for restocking the cart afterward catheter insertion, enabling the proper expensing of the procedure and replacement of the cart to the respective unit of measurement housing the cart. With the assistance of the marketing section, the facility printed advisory brochures reinforcing the importance of hand washing. The brochures were provided to all patients who were admitted to the facility in an endeavor to educate and increase health care provider compliance with the infection prevention process.
Once these interventions were in place, a root-cause analysis was performed on whatever infection identified. Equally infections were identified, cases were reviewed by the task forcefulness and the involved staff caring for the patient on a weekly footing. Each analysis evaluated the compliance with prescribed interventions and identified intendance practices requiring improvement in a arraign-free environment.
Side by side steps
Six months afterward these interventions were in place, a review of literature identified the use of CHG bathing every bit a supplemental strategy for the prevention of CLABSI. The strategy was brought to the task force for review, and it was decided the intervention would be trialed in 1 of the 3 adult ICUs. Following a 3-month trial of using a prepackaged 2% CHG bathing product, the practice was implemented in all adult ICUs. Twelve months before the initial trial, the Cardiac ICU had 2.half dozen infections per 1000 patient days. During the trial, their rate was 0.33 infections per one thousand patient days. The Medical ICU had a rate of 0.75 infections per 1000 patient days prior to the trial, which decreased to 0.33 infections during the trial. The Surgical ICU had a rate of 0.83 infections per 1000 patient days (nontrauma population) prior to the trial and 0.33 infections during the trial. The addition of CHG baths necessitated a modify in the facility central line policy. The policy was updated to include the bathing protocol in the adult ICUs. During the aforementioned time period, the use of CHG impregnated catheter caps was as well introduced in the ICUs.
Shortly thereafter, the focus of the chore force turned to the medical-surgical nursing units. But 4 of those units had an infection rate below the national benchmark during 2011.30 On the basis of the lower cost of the CHG bathing production compared to the CHG impregnated caps, ease of use, and the potential for a big impact on infection rates, the task strength decided to forgo implementing the CHG impregnated caps and that the next step needed to be implementation of the CHG bathing process in the medical-surgical units.
CHG bathing process
The daily CHG bathing process was introduced in all of the medical-surgical units for patients who had a central line. The facility chose to utilize prepackaged wipes that were impregnated with a ii% CHG solution at a cost of $5.77 for each package. Equally this was something most patients would accept been unfamiliar with, nursing staff were coached on how to explain the new procedure to patients and their families. To maximize the effectiveness of CHG bathing and to ensure consistency between staff, stride-by-step instructions of the bathing procedure were taught in the mandatory staff inservice programs and provided on a laminated bill of fare that they could refer to during the bathroom. The inservices were attended by all registered nurses and nurses' aides. Steps included using soap/shampoo and water to clean the face, hair, and genital surface area rather than the CHG wipes and then to cleanse the patient'due south torso from jaw line to feet. One fabric was to exist used for each of the 6 torso areas: neck, shoulder, and breast; upper extremities; abdomen; right lower extremity; left lower extremity; and back and buttocks. Skin was not to exist rinsed and needed to air dry out completely.
Although implementing the CHG baths was the chief intervention, simultaneous back up strategies were implemented to maximize quality outcomes. Those 4 strategies included staff education, making sure there was strong leadership back up, ensuring availability of resources, and increasing staff sensation and accountability.
Support strategies
Prior to implementing CHG bathing in the medical-surgical units, comprehensive education was provided to all nursing staff. Ane-hour pedagogy sessions were held on each unit for each shift and consisted of a review of the production, the rationale underlying the practice, an explanation and demonstration of the technique, and a competency exam. This content was also integrated into new employee orientation sessions and was added equally a component of the yearly skills competency cheque-off. The task force identified the demand for strong leadership support to solidify the QI procedure. In the past, staff did not receive feedback when patients developed infections on their corresponding nursing units. Unit leaders would be required to share the procedure comeback results with their staff, and quality measures such as CLABSI rates would become a part of annual evaluations of all nursing leadership, from the nursing unit manager to the chief nurse officer.
Implementing CHG bathing would require additional supplies for each unit. The units' operational budgets were adjusted to accommodate the increased price of stocking CHG wipes, and units with higher insertion rates were provided with additional central line insertion carts. To increase staff awareness and accountability of their part in prevention of BSI, direct care nursing staff would be included in root cause analysis investigations. Beyond increasing each participating nurse's awareness of the specific CLABSI occurrence, "lessons learned" could exist taken back to the private units as another means to educate and engage staff in the QI projection.
In addition, "visibility walls" have been placed in public areas on individual nursing units as a method to increase staff and public sensation of nursing sensitive indicators and back up the culture of transparency. Each unit places its unit-specific results for quality initiatives such equally falls, pressure ulcers, patient experience, catheter-associated urinary tract infections, and CLABSI on the wall. National benchmarks and unit of measurement results are displayed in piece of cake-to-read graphs. Early evaluation of this strategy has revealed that the visibility wall has become a source of pride for staff and that they have developed a growing sensation and accountability for their role in improving outcomes. Ongoing compliance efforts include daily review of the medical records and auditing for documentation of chlorhexidine bathing and cardinal line care.
RESULTS
Eight months into this project, formal tracking of the standardized infection ratio for each medical-surgical unit of measurement continues to exist monitored. Before interventions such as staff education (use of preinsertion checklists, charting line maintenance, and mitt hygiene); electronic medical tape triggers; and central line insertion supply carts remain in place. Ongoing medical record audits assure CHG bathing compliance. Since implementing CHG baths, a downward tendency in the overall number of central line infections in the medical-surgical units has been observed. Over this 8-month flow, 8 CLABSIs take been recorded (a charge per unit of 0.52 infections per 1000 patient days), compared to a total of 17 (a charge per unit of 1.46 infections per 1000 patient days) over the previous 12 months. Table 2 presents CLABSI rates for the pre- and post-CHG implementation for the 8 medical surgical units participating in the procedure improvement projection.
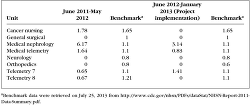 | Tabular array two. Medical-Surgical Units' CLABSI Rates Pre- and Post-CHG Implementation |
Word
Throughout the implementation project, the chore forcefulness has continued to review each case of key line infection and identified areas for connected improvement. Problems identified with recent infections include inconsistencies in line maintenance practices, inadequate manus hygiene, and variability of unit of measurement auditing practices. A standardized process by which each unit audits compliance of the central line maintenance and bathing practices is currently existence developed and will be included in the facility central line policy. A renewed and vigilant focus on hand hygiene has also been identified equally a priority.
Results from this QI project suggest that the implementation of CHG baths for non-ICU patients with key lines is an effective exercise change. The occurrences of CLABSI in these units decreased more than 50% over the previous yr. This experience demonstrates the value of using a QI process that identifies issues, aids in developing a comprehensive plan that includes all major stakeholders, and builds a process for ongoing evaluation with a ways for disseminating the results to staff, patients, and facility visitors.
The multidisciplinary chore force used a comprehensive review procedure to identify issues that may have contributed to the high CLABSI rates and worked to accost those issues prior to introducing CHG baths on the medical-surgical units. This first step helped build a comprehensive system that would broaden the introduction of CHG baths. Supporting strategies included staff pedagogy, garnering potent leadership support in implementing the bathing procedure, and providing continuous feedback of the results to staff. In addition, addressing the need for supplies for not simply the baths only besides for cardinal line insertions led to the resolution of a longstanding bulwark to consistent utilization of preinsertion checklists. The improver of specific triggers and documentation of line maintenance tasks to the electronic medical record improved the completeness and consistency of nursing documentation.
The goal of preventing CLABSI has challenged health care providers to develop innovative and comprehensive evidence-based practices. With this goal in heed, the facility accepted the claiming and identified a need in a susceptible population. Facilities need to systematically evaluate their care practices and ensure that high standards are existence achieved regardless of the patient's location in the facility. The process described in this article tin can be useful to others in undertaking similar QI projects at their facilities where adverse outcomes telephone call attention to a need for change, but no direct and standardized application process exists.
REFERENCES
1. O'Grady NP, Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. 2011;52(9):e162-e193. [Context Link]
2. Marschall J, Leone C, Jones Thou, et al. Catheter-associated bloodstream infections in general medical patients outside the intensive care unit of measurement: a surveillance report. Infect Control Hosp Epidemiol. 2007;28(8):905-909. [Context Link]
3. O'Horo JC, Silva GLM, Munoz-Cost S, Safdar N. The efficacy of daily bathing with chlorhexidine for reducing healthcare-associated bloodstream infections: a meta-analysis. Infect Control Hosp Epidemiol. 2012;33(3):257-267. [Context Link]
4. Hollenbeak CS. The cost of catheter-related bloodstream infections: implications for the value of prevention. J Infus Nurs. 2011;34(v):309-313. [Context Link]
5. O'Grady NP, Alexander G, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections, 2011. Centers for Affliction Control and Prevention. http://www.cdc.gov/hicpac/pdf/guidelines/bsi-guidelines-2011.pdf. Published Apr 1, 2011. Accessed July 24, 2013. [Context Link]
vi. Climo M, Diekema D, Warren D, et al. Prevalence of the use of central venous access devices within and outside of the intensive care unit of measurement: results of a survey amidst hospitals in the prevention epicenter program of the Centers for Affliction Command and Prevention. Infect Control Hosp Epidemiol. 2003;24(12):942-945. [Context Link]
7. Kusek 50. Preventing key line-associated bloodstream infections. J Nurs Care Qual. 2012;27(4):283-287. [Context Link]
8. Popovich KJ, Lyles R, Hayes R, et al. Human relationship between chlorhexidine gluconate skin concentration and microbial density on the pare of critically ill patients bathed daily with chlorhexidine gluconate. Infect Command Hosp Epidemiol. 2012;33(9):889-896. [Context Link]
9. Kasskian SZ, Mermel LA, Jefferson JA, Parenteau SL, Machan JT. Bear on of chlorhexidine bathing on hospital-caused infections amidst general medical patients. Infect Control Hosp Epidemiol. 2001;32(3):238-243. [Context Link]
10. Popovich KL, Hota B, Hayes R, Weinstein RA, Hayden MK. Effectiveness of routine cleansing with chlorhexidine gluconate for infection prevention in the medical intensive care unit of measurement. Infect Command Hosp Epidemiol. 2009;30(x):959-963. [Context Link]
11. Karki S, Cheng Air conditioning. Impact of non-rinse skin cleansing with chlorhexidine gluconate on prevention of healthcare-associated infections and colonization with multi-resistant organisms: a systematic review. J Hosp Infect. 2012;82(two):71-84. [Context Link]
12. Yokoe DS, Mermel LA, Anderson DJ, et al. Executive Summary: a compendium of strategies to prevent healthcare-associated infections in acute care hospitals. Infect Control Hosp Epidemiol. 2008;29(1):S12-S21. [Context Link]
xiii. Marschall J, Mermel LA, Classen D, et al. Strategies to prevent key line-associated bloodstream infections in acute care hospitals. Infect Control Hosp Epidemiol. 2008;29:S22-S30. [Context Link]
14. Edwards JR, Peterson KD, Andrus ML, et al. National Healthcare Prophylactic Network (NHSN) written report, data summary for 2006. Am J Infect Control. 2008;36:609-626. [Context Link]
xv. Lio PA, Kaye ET. Topical antibacterial agents. Med Clin North Am. 2011;95(4):703-721. [Context Link]
xvi. Ritz J, Pashnik B, Padula C, Simmons 1000. Effectiveness of 2 methods of chlorhexidine bathing. J Nurs Care Qual. 2012;27(2):171-175. [Context Link]
17. Bleasdale SC, Pull a fast one on WE, Gonzalez IM, Lyles RD, Hayden MK, Weinstein RA. Effectiveness of chlorhexidine bathing to reduce catheter-associated bloodstream infections in medical intensive care unit of measurement patients. Arch Intern Med. 2007;167(19):2073-2079. [Context Link]
18. Climo MW, Sepkowitz KA, Zuccotti Grand, et al. The effect of daily bathing with chlorhexidine on the acquisition of methicillin-resistant staphylococcus aureus, vancomycin-resistant enterococcus, and healthcare-associated bloodstream infections: results of a quasi-experimental multicenter trial. Crit Care Med. 2009;37(vi):1858-1865. [Context Link]
19. Munoz-Price L, Hota B, Stemer A, Weinstein RA. Prevention of bloodstream infections by use of daily chlorhexidine baths for patients at a long-term acute care hospital. Infect Control Hosp Epidemiol. 2009;30(xi):1031-1035. [Context Link]
xx. Dixon JM, Carver RL. Daily chlorhexidine gluconate bathing with impregnated cloths event in statistically significant reduction in key line-associated bloodstream infections. Am J Infect Control. 2010;38(x):817-821. [Context Link]
21. Evans HL, Dellit TH, Chan J, Nathens AB, Maier RV, Cuschieri J. Effect of chlorhexidine whole-trunk bathing on hospital-caused infections among trauma patients. Arch Surg. 2010;145(three):240-246. [Context Link]
22. Lopez AC. A quality comeback program combining maximal barrier precaution compliance monitoring and daily chlorhexidine gluconate baths resulting in decreased central line bloodstream infections. Dimens Crit Care Nurs. 2011;xxx(5):293-298. [Context Link]
23. Montecalvo MA, McKenna D, Yarrish R, et al. Chlorhexidine bathing to reduce key venous catheter-associated bloodstream infections. Am J Med. 2012;125:505-511. [Context Link]
24. Climo MW, Yokow DS, Warren DK, et al. Effect of daily chlorhexidine bathing on hospital-caused infection. N Engl J Med. 2013;368(six):533-542. [Context Link]
25. Lee A, Harlan R, Breaud AR, et al. Blood concentrations of chlorhexidine in hospitalized children undergoing daily chlorhexidine bathing. Infect Command Hosp Epidemiol. 2011;32(iv):395-397. [Context Link]
26. Centers for Disease Command and Prevention. April 2013 CDC/NHSN protocol corrections, description, and additions. http://www.cdc.gov/nhsn/pdfs/pscmanual/4psc_clabscurrent.pdf.-> Accessed May 20, 2013. [Context Link]
27. Clancy CM. Getting to nix: our efforts to eliminate infections nationwide. J Nurs Care Qual. 2010;25(three):189-192. [Context Link]
28. Lukas CV, Holmes SK, Cohen AB, et al. Transformational alter in health care systems: an organizational model. Wellness Intendance Manage Rev. 2007;32(four):309-320. [Context Link]
29. Moen R, Norman C. Evolution of the PDCA cycle. http://pkpinc.com/files/NA01MoenNormanFullpaper.pdf. Accessed July 24, 2013. [Context Link]
30. Dudeck MA, Horan TC, Peterson KD, et al. National Healthcare Prophylactic Network (NHSN) report, data summary for 2011, device-associated module. National Center for Emerging and Zoonotic Infectious Diseases. Division of Healthcare Quality Promotion. http://world wide web.cdc.gov/nhsn/PDFs/dataStat/NHSN-Report-2011-Data-Summary.pdf. Accessed May xx, 2013. [Context Link]
central line-associated bloodstream infection; chlorhexidine bathing; infections; quality improvement
dulaneythereoper1965.blogspot.com
Source: https://www.nursingcenter.com/journalarticle?Article_ID=1700151&Journal_ID=54010&Issue_ID=1699969
0 Response to "A Committee of Nurses Have Been Tasked With Reviewing an Increase in Central Line Infections"
Post a Comment